

On May 25, the world welcomed a special baby boy. Measuring 49 centimeters and weighing slightly more than three kilograms, he was the first infant born worldwide following a uterus transplantation performed through a robot-assisted surgery on both donor and recipient. The breakthrough was made possible thanks to years of research by the University of Gothenburg (GU), Sweden.
- The University of Gothenburg is at the forefront of the research on robot-assisted uterus transplants;
- Operating with robots is less invasive and causes less post-operative discomfort to patients;
- Augmented Reality, bioengineering, and AI might be the next technologies to enter operating theaters;
Conceiving, carrying, and giving birth is one of the deepest desires for couples, but for women that don’t have a functioning uterus – either because their womb can’t bear pregnancy or because they don’t have one – having a child is nearly out of reach. Following the introduction of in-vitro fertilization in the late 70s, science has paved the way for giving every woman the right to be a mother. Robots are helping doctors ease transplantations.
The birth of a baby from a fully robot-assisted transplant is the last of many accomplishments by the University of Gothenburg research team. Since 1999, it has been investigating uterine transplants. In 2012, the first transplant happened, followed by the first birth in 2014. The doctors started with robot-assisted keyhole surgery three years later, which led to the first births in 2021.
Dr. Niclas Kvarnström and Dr. Mats Brännström, respectively, a transplant surgeon at the Sahlgrenska University Hospital – GU’s medical center – and professor of obstetrics and gynecology at Sahlgrenska Academy, told Innovation Origins more about their research.
How does a robotic-assisted intervention work?
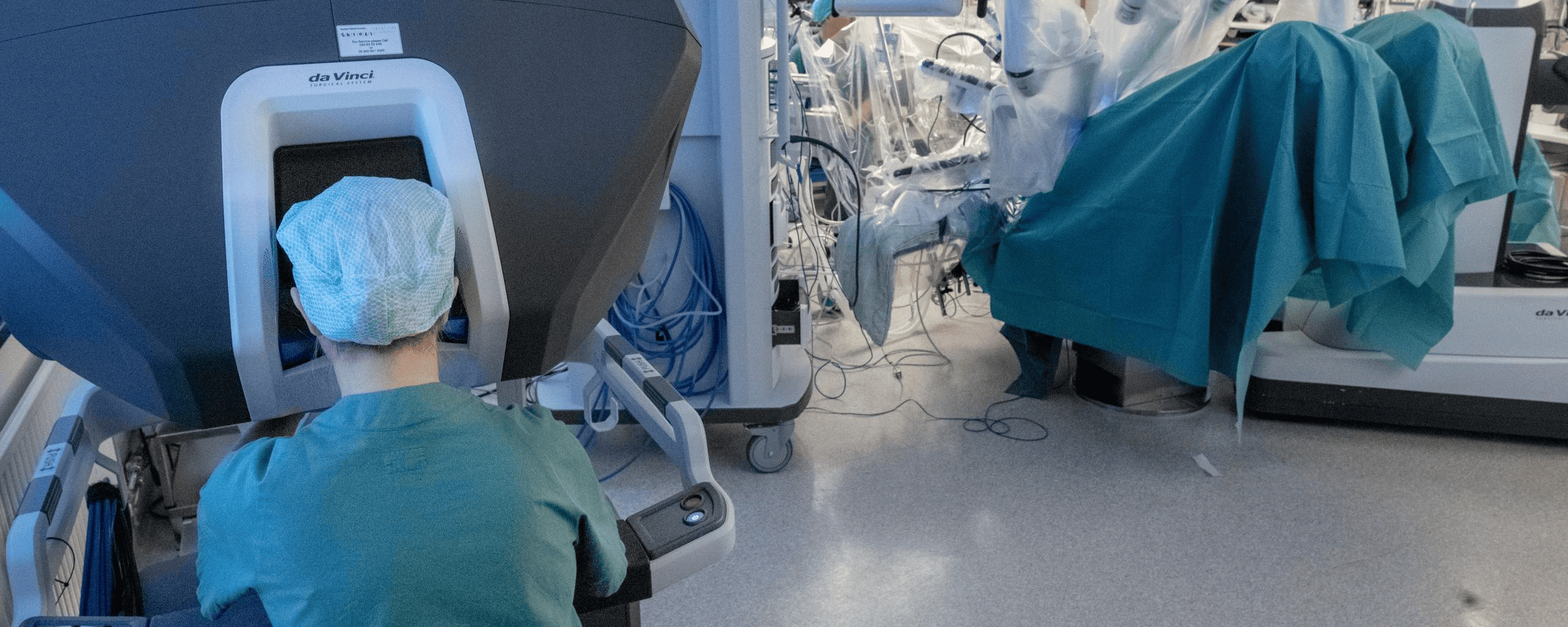
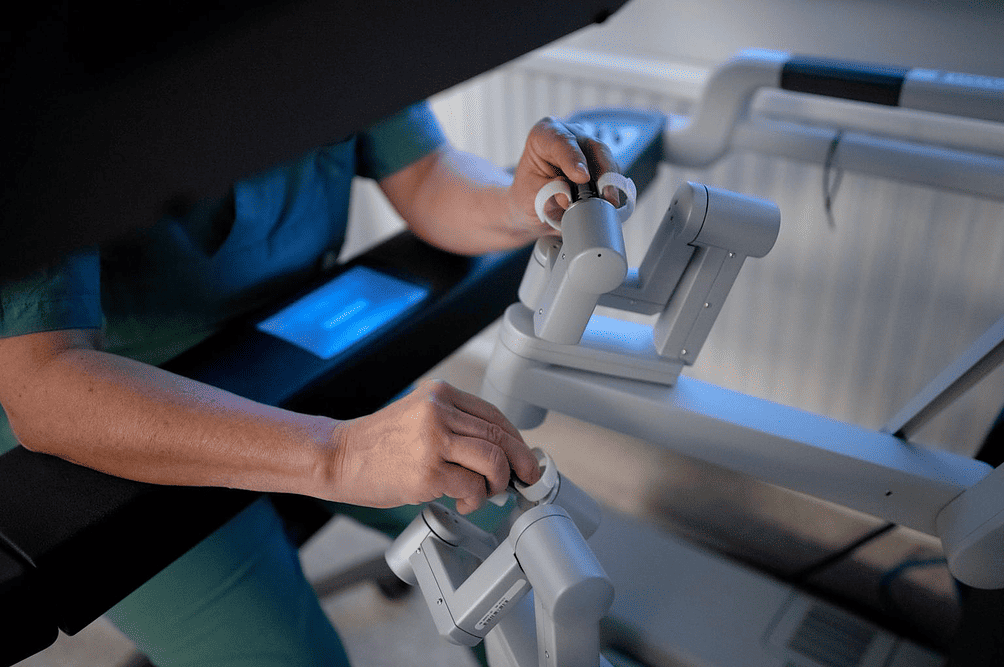
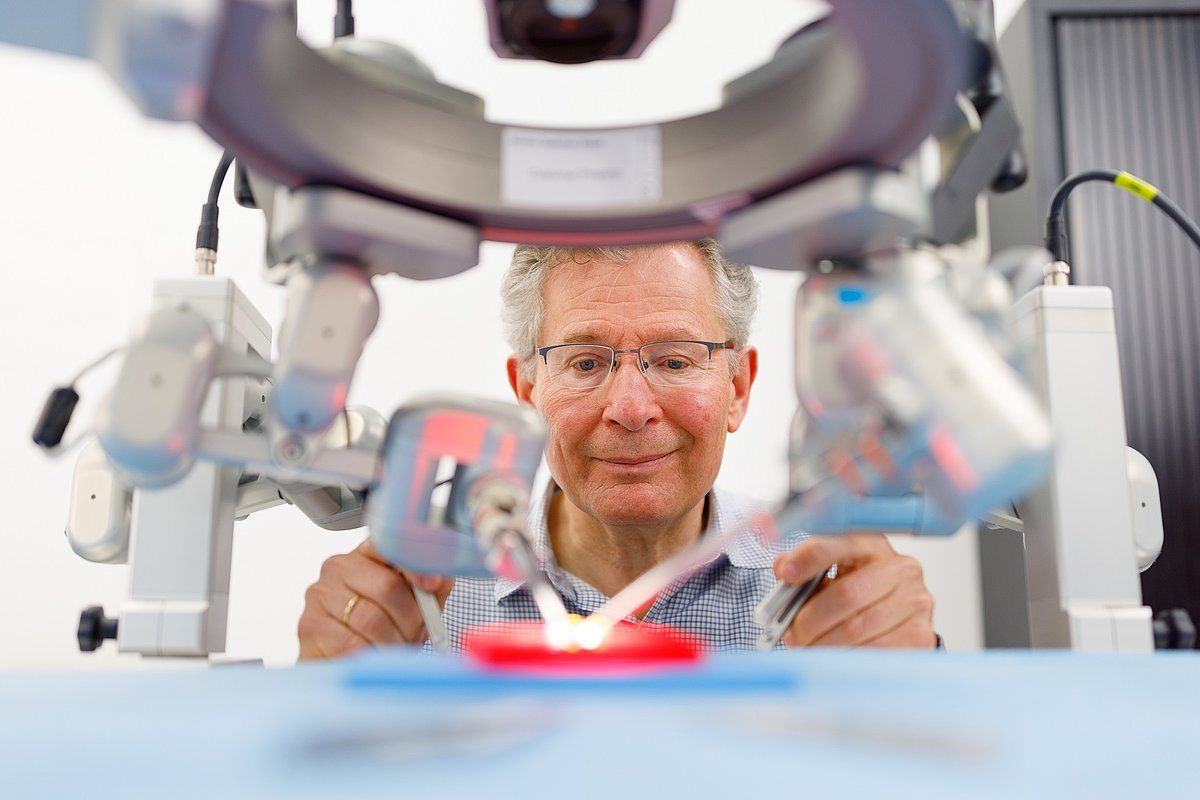
Robot surgery allows for less invasive interventions than conventional open surgery. This technology inserts cameras and robotic arms having surgical instruments through small holes in the lower belly. From the operating station, they can get high-quality pictures of the body area they are working on. Through joystick-like controllers, doctors can move surgical tools with high precision. “You don’t make any mistakes, as you can see exactly where the needle is coming in and out,“ says Kvarnström.
Hand movements are scaled-down when using the joysticks. “Making wide movements results in actually small actions in the operating field. That’s how you can be very precise,‘’ adds Kvarnström. Minimizing interventions, in turn, gives patients less post-operatory discomfort.
Reducing drug intake
In further reducing post-intervention pain, robotic surgeries reduce the risk of adhesion formations. An adhesion is the body’s repair mechanism response to tissue disturbance – such as trauma, surgery, or infection – that, in the form of a band of scar tissue, attaches two parts of tissue that usually are not joined together.
“Having fewer of them helps when the baby is delivered. In addition, the uterus graft is removed after bearing one or two pregnancies,” explains Kvarnström. Following the transplant, receivers are subministrated drugs to prevent reactions from the body. As with every other medicine, these come with side effects, and long-term use can be dangerous.
Touch
If there’s one thing that robots can’t replicate (yet) as opposed to laparotomy – the surgical procedure of opening the abdominal cavity to expose organs – it is feeling tissues. Laparotomy was the technique used in the first non-robotic transplants. “The great advantage of laparotomy is ‘having the hands in the field,’ which is feeling the tissues and the structures, whereas, with robotics, it’s a mere visual process,” says Brännström.
However, he’s confident that as more manufacturers emerge, next-gen robots will have the sensitivity, too. For instance, embedding sensors on the operating instruments to provide feedback on applied pressure might be a way.


Robots to disrupt healthcare
Nevertheless, robots are changing the profession in many ways. In addition to diminishing post-operatory patient discomfort, it’s easier to train the next generation of surgeons to perform procedures. As less pain is created for patients, discharging times are reduced, too, thus curtailing hospitalization costs.
Robots still come at a high price tag, so they can’t be everywhere. Investing in them – the standard da Vinci surgical robot comes at $2 million – might have more significant effects. “It may be cost-effective for hospitals and the whole society, too. It’s a big difference if a woman takes a one-week or six-week sick leave. In calculating the costs involved in a transplant, we discovered that sick leave-related ones are 35 percent of them,” explains Brännström.
Perfecting the method
After achieving another milestone, the Sahlgrenska University Hospital will keep investigating the matter. “The next step is learning when to apply this procedure and when not to. In our case, we want to have it in our portfolio of the procedures we can offer, but at the moment, we still need to explore and figure out in what cases it works best,” underlines Kvarnström.
Operating times remain a constraint, though. Taking the uterus from the donor through the robot procedure can take up to ten hours, adding to the eight hours needed to transplant the graft. “Niclas [Dr. Kvarnström] is possibly sitting using the robot for up to 15 hours, an unbearable span of time if standing up,” emphasizes Brännström. Nonetheless, both doctors believe that operating times can be reduced with practice.
What technology will enter the operating theater next?
As the GU stays at the forefront of research and technology adoption, other innovations have the potential to reach operating theaters soon. Kvarnström suggests that augmented reality (AR) can impact the future of surgery, as it would allow displaying relevant information during the procedure.
Brännström goes even further. “The next big thing will be uterus bioengineering.” This discipline applies engineering concepts to biological systems to design bacteria, organs, or tissues. Bacteria engineered to produce specific chemicals are an example. One of the advantages is the possibility of creating organs ad hoc for each patient. “Uteruses would be created in the lab using stem cells without needing to take them from humans. It will still take time, as it’s still being experimented on rats and rabbits,” he says.
Eventually, AI will also reach operating theaters as more data will be amassed to train algorithms. The future is bright, as technology can help satisfy one of the most profound human desires: being a mother and father.
Related Posts





