

Premature babies in incubators, COPD patients, and people with acute lung disease in the ICU. All of them suffer from hypercapnia: elevated CO2 levels in the blood. When a patient has breathing difficulties, you tend to think fairly soon of an oxygen deficiency. But in hospital, inserting a tube into the nose often fixes that in no time. “When someone starts having difficulty breathing, it’s usually down to the accumulation of CO2. That CO2 is supposed to be exhaled, but then that process gets disrupted. This is how the body poisons itself with carbon dioxide, so to speak,” says Richard Ramakers, CEO of O11 biomedical.

Brainstorming at a bar
Adherence to treatment among COPD patients is problematic. People need to use the correct inhalation technique at home and use their inhaler on time. Patients who do not use their medication optimally are more likely to be hospitalized, have a lower quality of life and a lower life expectancy. Acute treatment of patients in intensive care with an artificial lung (ECMO) is subject to frequent and life-threatening complications, such as internal bleeding. This is why O11 is developing a liquid breath (RESPILIQ™) that patients can drink from a packet.

The idea was born when co-founder and CSO Stefan Jockenhövel attended a congress on this form of therapy 20 years after receiving his PhD for his research on heart lung machines for babies. He saw that the treatment still carried numerous risks. Ramakers: “Then he sat down in a bar with a jug of beer. That’s when he came up with a solution where the excess CO2 is discharged through the intestines.”
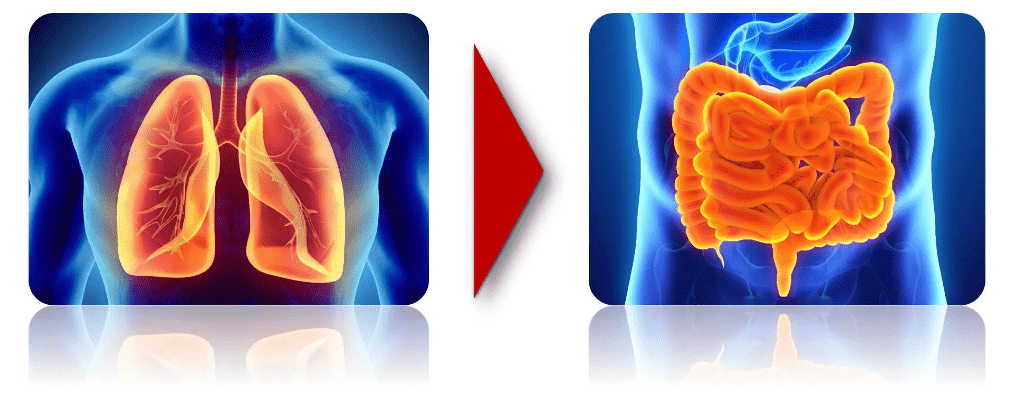
Intestines as an exchange membrane for carbon dioxide
That solution didn’t just magically appear out of nowhere. Doctors first started using colonoscopies in the 1960s. In this examination, the doctor uses a flexible tube to examine the inside of the intestines. This involves pumping a measure of carbon dioxide gas into the tube to slightly inflate the bowel. “Then they noticed that the level of carbon dioxide in the blood immediately goes up when you blow carbon dioxide into the intestine. The intestine consequently causes the carbon dioxide gas to be absorbed into the blood.”
That the intestines proved to be a good exchange membrane for carbon dioxide gas was actually a side effect of this research. Until Jockenhövel came up with RESPILIQ™ together with co-founder and pulmonologist Christian Cornelissen at Forckenbeck café on the Aachen campus. The drug is contained in a drink packet, its contents resemble semolina porridge with little chunks. The major difference is that the chunks in RESPILIQ™ are not clods of flour but plastic globules that have the ability to absorb CO2 when they reach the intestines.
Clearing up CO2
“The liquid ends up in the intestines. There is too much carbon dioxide gas in the blood of our patient group. Since the intestinal wall lets this gas pass through, the intestinal fluid also has too much carbon dioxide. Our globules absorb CO2 from that intestinal fluid. As a result, there is less carbon dioxide in the intestinal fluid, creating a CO2 pressure difference with the blood. This in turn causes the blood to expel its excess carbon dioxide into the intestines,” Ramakers explains. In this way, liquid breath helps the body to get rid of accumulated CO2 and patients can breathe more easily.
‘A secret trick’
The tiny globules are made up of a type of polymer in which an absorber is encased. Ramakers does “a trick with them,” but that will remain a trade secret. With three of these packets of liquid breath a day, a COPD patient (and there are over 600,000 of them in the Netherlands alone) should be able to lead an active life.
Ramakers emphasizes that the drug is still under development. When he appeared on German television a few weeks ago, he immediately had several COPD patients calling him the following day. “People all over Europe Googled us. I can always hear immediately if I have a patient on the line. Their voice sounds hoarse but hopeful; they are literally gasping for breath.”
The other day, an investor asked Ramakers if the liquid actually tastes nice. “A question that only occurs to healthy people. Adherence to treatment is currently a major problem for COPD patients. We expect to solve this problem with our drug. All you have to do is drink it. It’s almost like an addiction; if you don’t drink it, you go into respiratory distress.
“People all over Europe Googled us. I can always hear immediately if I have a patient on the line. Their voice sounds hoarse but hopeful; they are literally gasping for breath.”
Richard Ramakers
The ICU as an ideal testing ground
On the very first attempt, O11 already had a medication that worked, although it will take another four years at least before the drug is available to COPD patients. It is a completely new therapy that must first be fine-tuned and satisfy all kinds of strict safety requirements. On top of that, the European approval process for the Medical Device Regulation (MDR) was overhauled last year. All medical devices have to be accredited all over again. “All of the agencies that are allowed to issue this kind of accreditation are completely full. It’s really a challenge to avoid delays,” Ramakers notes.
The plan is to first demonstrate in an ICU in Germany that the medication does what it promises. This is a manageable market where the start-up will not need its own logistics company. A patient spends up to two weeks in the ICU and is monitored very intensively, which makes it a great testing ground. “When we launch ourselves on the COPD market, the big question is: who do you help, and who are you not going to help? Also, it’s more difficult to actually get the medication to the actual patient. And once a patient starts using it, they will be dependent on it for the rest of their lives. Then you have got to have extremely reliable logistics and supplies.”
The best of both worlds
Ramakers quit his job at the Aachen-Maastricht Institute for Biobased Materials (AMIBM) in January. He then served as director of the institute for five years. These days, O11 is renting a space in the start-up loft of the campus and finding out what it is like to use the facilities of the Brightlands Chemelot Campus and AMIBM as an entrepreneur.
“Our partner AMIBM has loads of facilities. These range from a vice to an extruder. If we, as a start-up, had to buy all that ourselves, we would be bankrupt before we had even started. Moreover, when we invite a customer, we are able to do that in a very representative space on campus, instead of a garage behind a house. That’s also another important motivation for being here.”
The start-up also has an office at the Institute of Applied Medical Engineering in Aachen and is trying to combine the best of both worlds. “In Aachen, we are able to do in vitro and in vivo tests like we can do nowhere else, and at the Brigthlands Chemelot Campus we work on plastics the way we wouldn’t be able to anywhere else.”
Collaboration
Related Posts





