

Normal life is virtually impossible for most dialysis patients. In addition to the constant discomfort and fatigue, there is the need to spend hours at the hospital on dialysis several times a week. But there is light at the end of the tunnel: the Dutch Kidney Foundation (Nierstichting) is currently working with researchers from imec and others at the Eindhoven-based Holst Centre to develop a portable artificial kidney. This compact dialysis device – which fits into a cabin suitcase – could already make the lives of kidney patients around the world a lot more bearable. But the ultimate goal of these researchers lies one step further: the development of an implantable artificial kidney that could eventually make the invasive treatment of kidney dialysis completely redundant.
It is still difficult to put a precise deadline on it, but the progress so far shows that it is a realistic ambition, says Fokko Wieringa, responsible for research into the artificial kidney at imec. The more compact solution that the Kidney Foundation plans to present before the end of the year is the first step, he says. “But in the meantime, for the longer term, we are already working towards a device so small that it can eventually be implanted.” The role of the electric blood pump – essential in a traditional dialysis machine – would then be taken over by the heart and the waste products would leave the body through the urine, just like a real kidney would operate.
In his ambitions, Wieringa adheres to Moore’s Law, which states that technological innovation in computer chips leads to the doubling of computing power every 12 months. The result: computers you can put in your pocket, which used to require entire halls. “If we realize a roadmap for international cooperation as we did in the chip industry, then you will have a usable implantable artificial kidney within fifteen years or so,” Wieringa predicts. “The result won’t be depending on the electronics, as imec is already proving. Partly thanks to ASML’s EUV lithography, an incredible amount of electronics can be put on a square millimeter. And the Netherlands is also very strong in the field of Organs-on-a-chip, where living cells and chip technology work together. Combine those two strengths and you’re at the global forefront.”
Tradition
Sensational innovation regarding kidney health fits into a Dutch tradition. Indeed, the Dutch physician Willem Johan Kolff stood at the cradle of the very first hemodialysis machine and saved the first patient with acute kidney failure in Kampen on September 18, 1945. Since then, hemodialysis has saved millions of lives, but this mechanical blood purification system is by no means perfect. Moreover, the equipment essentially has changed very little in the last 50 years. Most people with kidney failure still have to visit a clinic several times a week for a treatment that is incredibly exhausting.
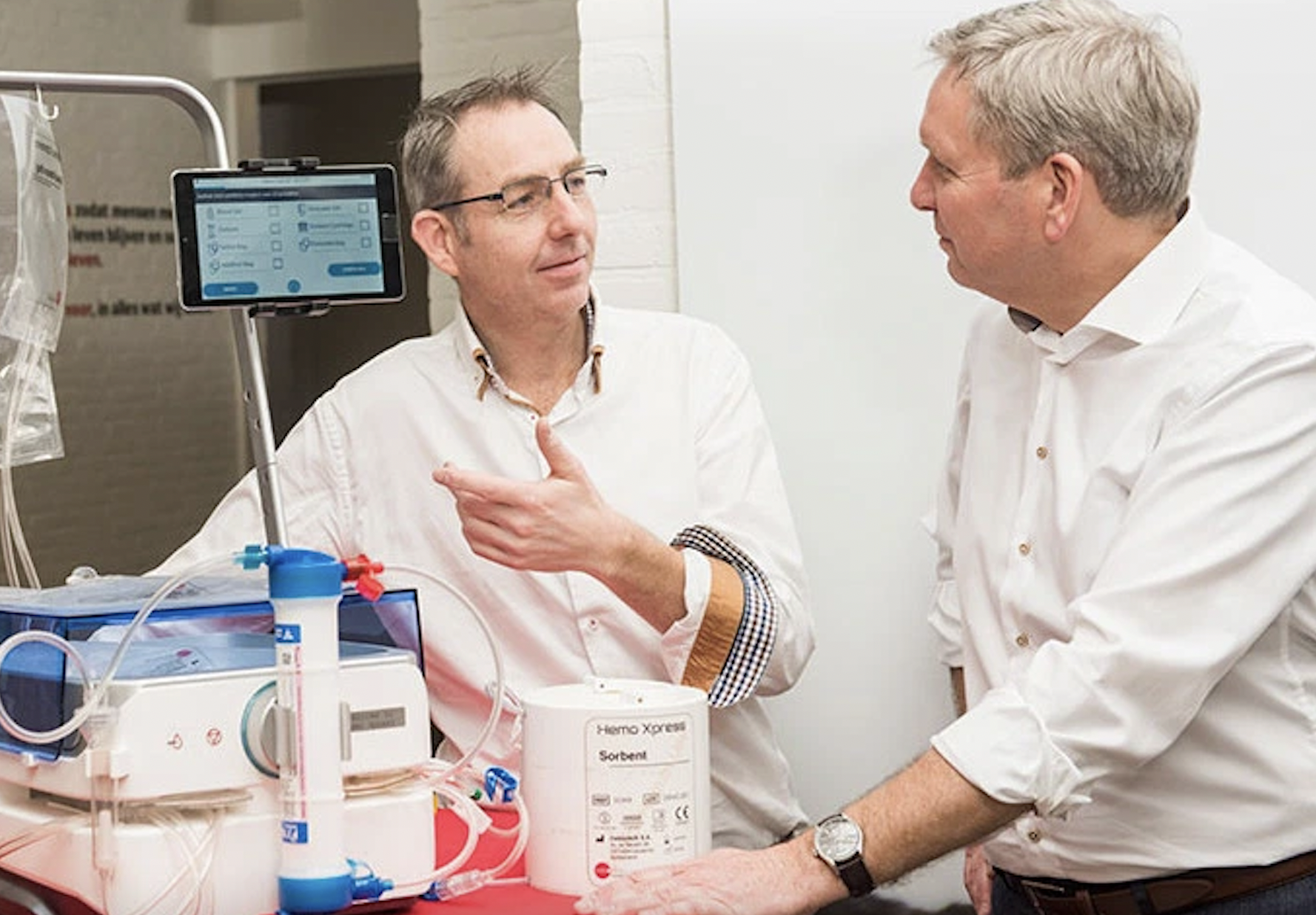
Meanwhile, the Kidney Foundation has been working for several years on a compact dialysis machine, so small that it can be taken on an airplane as hand luggage. This required several breakthroughs, but with the help of researchers from Holst Centre in Eindhoven, Debiotech from Lausanne, AWAK Technologies, Dialyss from Singapore, and a number of Dutch health insurers, developments have suddenly moved fast in the last 5 years, says Jasper Boomker of the Kidney Foundation.
The Dutch/Swiss company NextKidney was founded, which can show the first prototype later this year, according to Boomker. Together with the UMC Utrecht, these organizations are working hard to prepare for the clinical tests that will take place in 2022. The device is easy to connect to any ordinary power outlet (even ungrounded). Moreover, unlike classic dialysis equipment, it does not require 70 – 120 liters of water, but 6 liters is enough.
What does a kidney actually do?
A dialysis device or artificial kidney partially takes over the function of a real kidney. But what do the kidneys do in the body?
Every person has two kidneys, each consisting of a complex grid of hundreds of thousands of tiny filters called nephrons. Those nephrons purify the blood and ensure its constant balance and quality. The filtered out toxins, such as urea, leave the body through the urine, while useful substances that we still need are recycled by the kidney. These include vitamins, minerals, salts, water, and glucose.
In many kidney diseases, however, this purification works less and less well, which eventually – if the kidneys work for less than 15% – is fatal without dialysis or kidney transplant.
Transplant
Currently, according to Boomker, the best treatment for kidney failure is the transplantation of a donor’s kidney. “But unfortunately we all know that there is a great shortage of these,” he says. So kidney patients remain mostly dependent on bulky and expensive blood dialysis machines that, despite their size, do not work nearly as efficiently as a real kidney.
One of the disadvantages of such a device is that in 3 treatments of 4 hours you try to “catch up” with the purification work that the kidneys do continuously 24 hours a day. That puts a particularly heavy burden on the heart, says Wieringa. “It’s also not really environmentally friendly when you consider the amount of electricity and water required for current equipment.”
Like Boomker, Wieringa has been involved in the project to drastically improve dialysis equipment for some time. Until 2017 this was from TNO in Delft and then from imec at Holst Centre, where they have the knowledge to use nanotechnology to make electrical devices ever smaller. NextKidney’s portable artificial kidney could turn an entire industry on its head, Wieringa says. A “disruptive technology,” in other words, similar to the electric car or the Internet. “This can improve and save the lives of many people, by also serve countries with poor infrastructure. And if we then push forward even further with an implantable artificial kidney, the social impact becomes greater again.”
Less water
“One of the main goals was to develop an artificial kidney that requires less water,” Boomker says. Dialyss, a spin-off company from the Singaporean Temasek Polytechnic, had a potential solution: sorbent technology. Temasek’s technology was already being used by the company AWAK for dialysis of fluid in the abdominal cavity. Dialyss was able to make the compact AWAK technology suitable for blood dialysis. “This allowed us to go from over 100 liters to 6 liters,” Boomker says.
The Swiss company Debiotech, together with imec and others, then went to work on the design of the smaller artificial kidney. “A dialysis machine is full of sensors,” explains Wieringa. “With our knowledge of nanotechnology, we are able to make those sensors and other electronics very small.” The importance of those sensors can hardly be overstated, says Wieringa. Not only does the quality of the blood have to be measured, but the patients themselves also have to be continuously monitored when they are on dialysis at home at night, for example.
Wieringa gives the example of automatic needle alarms. “The worst form of blood leakage is when the return needle (which brings the purified blood back into the patient) detaches, while the machine continues to pump blood out of the patient via the other needle, which ultimately can lead to death. Within its activities at Holst Centre, imec has achieved international recognition within its activities at Holst Centre for sensor technology that immediately sets off an alarm and also stops the blood pump as soon as blood leaks.”
And so, according to Wieringa, there are more sensors that can make home dialysis just as safe as in the hospital. In principle, it would even be possible to monitor a patient completely remotely and, in the event of questions, to provide assistance by telephone or video link (even via the device itself).
In this project, Wieringa is also very concerned with the regulations surrounding equipment and medical services. “You can’t just develop a device and bring it to market. There are numerous standards that must be met. Committees have to look at the new technology and give their approval. It’s important to consider this very early in the development process and, above all, to let the patients’ voices be heard.”
Vested interests
An inhibiting factor here – and this applies to more disruptive technologies – is that a lot of persuasion is needed to get the “old” dialysis equipment manufacturers and regulators on board. Wieringa: “Don’t forget that this is an industry in which tens of billions of euros are involved, with high-profit margins, both for manufacturers of machines and clinics. Their support is crucial, however, because this is where the power lies to ultimately be able to make millions of portable artificial kidneys at the lowest possible price, with a global service.” The innovators have to overcome a double hurdle, so to speak: the recognition that the existing equipment may eventually cease to be used, in addition to the business risk surrounding the development of a new device.
And that’s not all, says director Tom Oostrom of the Dutch Kidney Foundation: “The reimbursement rates for current blood dialysis are under pressure worldwide, forcing the dialysis industry to adapt the current business model. What does help with this is the broad support for innovation in dialysis from the United States.”
Technical hurdles for NextKidney’s artificial kidney are few, according to Boomker. The main issues now are clinical trials and finding new investors. Like Wieringa and Oostrom, he is hopeful. “With this, the Netherlands can once again show the world how we can turn our technological expertise into usefulness for society.”
Related Posts





