

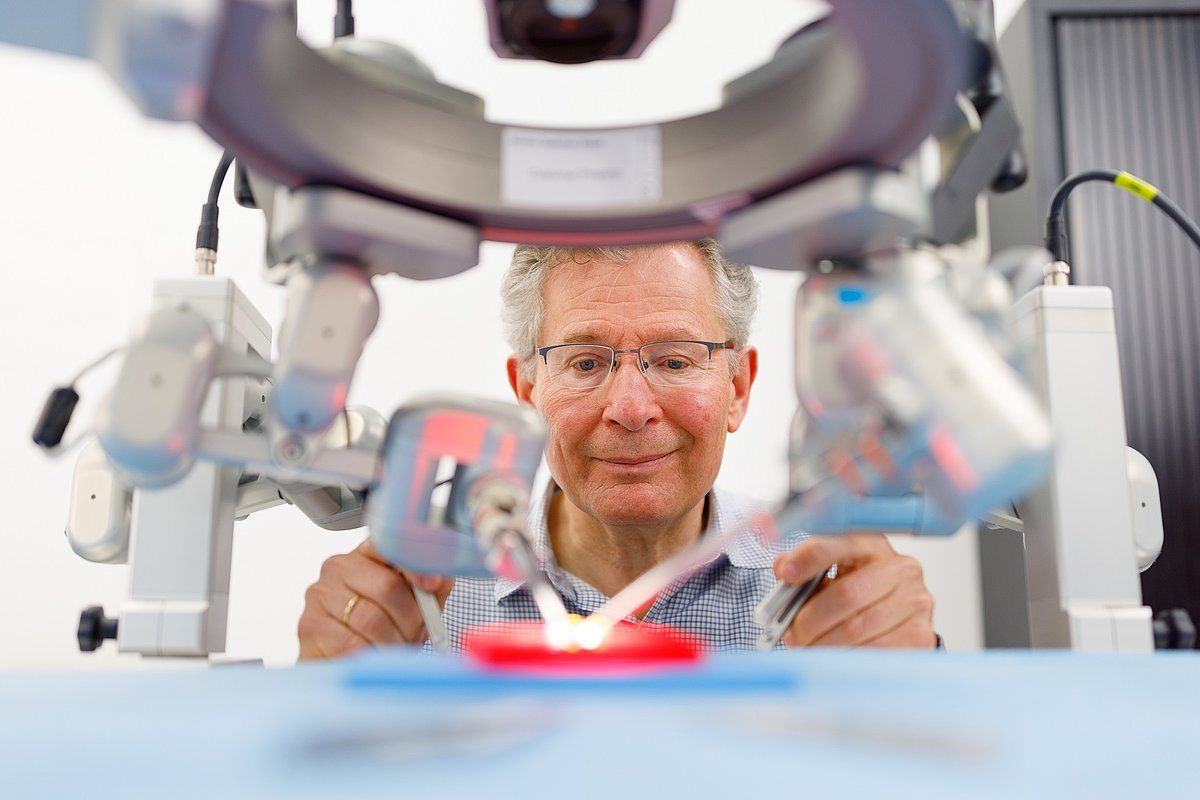
The world’s first microsurgery robot was “born” at the Brightlands Maastricht Health Campus. “I think we are entitled to be very proud of this”, says Tom van Mulken.
Born in Geleen, Tom van Mulken went to South Africa for his internships. His focus there was research on “penetrating injuries of the abdomen,” as this is so beautifully put. In practice, this appeared to be rather difficult: there was a container in the parking lot of the hospital in Soweto that doubled as a mini operating room where people with knife and gunshot wounds could seek treatment on the weekends. Van Mulken: “There were long lines every weekend, and there I was as an intern, stitching patients up who had been attacked by people wielding machetes. These were also the scenes we saw at the University Hospital in Johannesburg. In the Netherlands, we only see this once every few months. South Africa is a beautiful country, but in Johannesburg you can’t safely walk down the street or stop at a red light at night.”
About BRIGHT PEOPLE
To make tomorrow’s world a little more beautiful, cleaner and better, BRIGHT PEOPLE are indispensable. In this series, each month we interview a figurehead of the Brightlands Campuses. These purebred innovators talk about their mission and how they want to achieve it.
Read the other installments of this series here.
Married and father of three, Van Mulken remained in the Netherlands, but did end up in plastic surgery partly due to his experiences in South Africa. His training was followed by another one-year fellowship in Sydney, where he specialized in hand and wrist surgery.
Besides, he was given a very warm welcome at MUMC+. “There is a great atmosphere here, egos don’t matter; it’s all a bit more light-hearted here than in other departments, even though our people are very ambitious in their work.”
Restoration of form and function
He says he feels at home here, enjoys the sophisticated operations that are precise down to the square millimeter. “I like the fiddly aspects, particularly from the reconstructive angle. With burns or other injuries, you never know exactly what kinds of problems you will run into. You have to get creative and think in terms of problem-solving, and you see immediate results. We are responsible for the restoration of form and function, and give these back when patients have lost them. This is very satisfying. Of course, we also have our limitations; the perfect solution often doesn’t exist. We can never give someone back their breast in breast reconstruction procedures, or the face back to someone with burns, but we do rise to the challenge. With hand surgery, you can actually give people back the use of their hands.”
Initially I thought, like everyone does, that plastic surgery was about breast augmentations and lip injections. When I realized that these surgeons mostly do reconstructive work, I thought, ‘Oh, this is cool’
Tom van Mulken
Microsurgery
Fiddling, problem solving, innovative thinking; all of this is right up Tom van Mulken’s alley. It’s no wonder he was paying attention when the idea came along to develop a robot that could assist with these microsurgical operations. “Well, I was still in training and wasn’t really into research because it was often mostly done to spruce up your résumé. I traveled a lot for my education: Finland, England, Suriname and South Africa. My trainer, Professor Van der Huls, was involved with the first surgical robot that came to the hospital here in 2007: the Da Vinci Robot. It was mainly designed for exploratory abdominal surgery. It was also used for the first time for connecting blood vessels for breast reconstruction surgery. For the really intricate work however, microsurgery, this robot was too unwieldy, way too powerful.”
The arrival of the Da Vinci robot in the hospital prompted the question in several departments about the added value robots could offer, including in plastic surgery. We came in contact with TU Eindhoven purely by chance. They wondered if we could produce a robot for microsurgery. “I was sitting here, as an assistant, and thought, ‘This really makes sense and would be great. This could really help us move forward.’”
Gyro Gearloose in the basement
He got to work on this, together with Raimundo Cau, a TU Eindhoven student. They watched operations, worked out problems with those involved and each other, locked themselves in the TU basement “like Gyro Gearloose” and developed a robot that the TU student eventually also built.
The testing phase followed; first on mock blood vessels, then on live tissue. They got approval for the device, but then the research budget ran out. MUMC+ and TU decided to turn it into a spin-off company – Microsure – in order to secure funding. The two developers became Chief Technical Officer and Chief Medical Officer, supported by a part-time CEO. These days, the company employs 22 people. Van Mulken bowed out to avoid any conflicts of interest. To make a long story short: “I’m a doctor.” He is still involved as a clinical adviser with a stock portfolio.
“I learned a lot about the business side. As a doctor, it was never my goal to start my own business. Now I realize that this is actually where a lot of innovation comes from; you need each other. We were only able to come this far because we brought the world of technology and that of healthcare together in that TU basement. This is how ideas are born. I’m much more open to new devices coming on the market now.”
Less trouble with a poor night’s sleep
For the record, the robot does not perform the operations itself. It’s actually an instrument that the surgeon controls, and which helps make the surgeon’s hand more stable and precise. The vessels he must suture together during a reconstruction procedure are 1 to 2 mm in diameter on average. This is really precise work. In these types of surgeries, the surgeon looks through a microscope that magnifies the image of the vessels ten to twenty times. This makes a surgeon’s hand a limiting factor.
Van Mulken: “What does the robot do? It eliminates any tremors coming from the surgeon’s hand. Some people are less affected by tremors than others, but not enough sleep or stress can easily influence performance. The robot can also handle downscaling. With a fairly large movement of my own hand, I can have the robot execute an incredibly precise, small movement. This enables me to be very exact in my work, and cause less damage to blood vessels. This is actually the only thing the robot does. I think we came this far because we kept it very simple.”
Reattaching amputated fingers
Van Mulken expects that microscopes will only improve and eventually even be replaced by 3D cameras. All the same, this robot will still only be used for studies, even though it now has a CE mark. The first study involves lymphatic surgery: women with breast cancer often undergo surgery or radiation of their armpits that prevent fluid from flowing properly away from their arms. This causes their arms to become swollen and heavy, a condition called lymphedema. One solution is to create a bypass for the lymphatic vessels in the venous system. This is done using the robot since these vessels are less than half a millimeter in diameter.
The robot is also used in the reconstructive surgery of open-leg fractures, tumors, or other traumatic injuries in which the patient’s own tissue has to be replaced and the blood vessels reattached. The robot also helps with injuries to nerves in the hand, or injuries from glass or circular saws.

Technological advancement
Currently under development, the third generation of the MUSA robot is the only one that can be put into production without restrictions, and will be even more precise, in addition to being easier to use and compatible with every possible instrument and camera. “Advancements used to be made in medicine whenever a new type of surgery was developed. And I still believe that this is a very good thing. However, I think the most progress in recent years has been made in incorporating technology into medicine.”
“We recently performed a lower leg reconstruction with our micro-robot and a 3D camera. We were able to work at a comfortable distance, wearing 3D glasses to operate with the robot. This will be the future. Light will also play an important role in this. UV light allows you to see nerves or lymphatic vessels better, for example. These days, this light is already built into microscopes. You can also apply this technique with cameras, so you only see the lymph vessel in a wound. No more endless, frustrating searches for the vessel. You just put another filter on it and you can see where the vessels are.”
AI will move us forward
And we haven’t even touched on artificial intelligence (AI). “This is going to teach us to see blind spots. Based on the data from ten thousand operations, for example, AI will be able to tell you that you are applying too much pressure to one area. This will facilitate making certain decisions during an operation, and make predictions based on all of the operations you’ve done in the past. AI will also help in training. Doctors are now trained because there’s someone looking over their shoulder. This person tells them how to perform certain procedures. The beauty of a robot is that you can quantify the force you’re using or movements you make, so it’s ideal for use in training models. AI can make immediate corrections if necessary. All of this helps the training to be much more effective.”
Better quality
Will AI take over completely? “No, you will still have to be experienced, you have to be able to see the patient and assess the decision to operate. It’s not like someone just starting out will be able to perform the entire operation on their own.” Do you make fewer mistakes because of the technology? “Yes, I believe the quality of operations now is becoming better, and more stable. It means it won’t matter as much whether or not you’ve had a good night’s sleep or very little sleep.”
The robot project began in 2007. It takes a long time to go through all the procedures. Tom van Mulken: “At the time, I didn’t expect we would get this far and that it would take this long. Something like this takes a long time. Not just in terms of hours per week; you have to supervise projects like this while you’re at work. It really has been a team effort. It proves that win-win works.”






