

Delivering quality healthcare is becoming an increasingly complex puzzle, especially in sparsely populated border regions. Here, finding qualified staff is more difficult, and the lack of intensive care beds (the Netherlands) or sufficient medication (Germany) is more significant than in densely populated areas. And that while both countries have the highest healthcare spending and the highest percentage of physicians in the EU.
“So, we can conclude that the situation is unsustainable,” Caroline Fischer interjects. Therefore, hospitals in these regions need to rely much more on each other, believes the assistant professor of public administration and digital transformation at the University of Twente (UT). Also – no, especially – in sparsely populated border regions. “If we have learned one thing from the COVID pandemic, public health does not stop at the national border.”
Why this is important:
Sparsely populated border regions often face healthcare challenges. This article offers an innovative solution that aims to address these challenges. It offers insights into how hospitals are collaborating across borders and leveraging technology to improve healthcare access and efficiency.
Float pools
That is precisely what the BRIDGE project, which secured 1.5 million in funding in December, focuses on. Fischer leads the consortium, which, in addition to UT, consists of the Nijmegen software company NovioQ, Acute Zorg Euregio, the University of Münster and the university hospital of Münster. Part of the wider consortium are Medisch Spectrum Enschede and two regional hospitals: St. Antonius Hospital in Gronau and the regional hospital in Winterswijk.
The idea arose when Fischer analyzed “float pools” for healthcare personnel. “In healthcare, we face a chronic shortage of people. The flexible deployment of staff can partially solve that shortage. You can deploy a float worker in different places, depending on where there is demand.”

Using staff efficiently and better scheduling
The umbrella term is ‘resource pooling,’ which involves more flexibility in using personnel, hospital beds, ambulances, medicines, and where patients are treated. Although technology can take over care tasks, there are also gains to be made by using care personnel more efficiently and making better schedules.
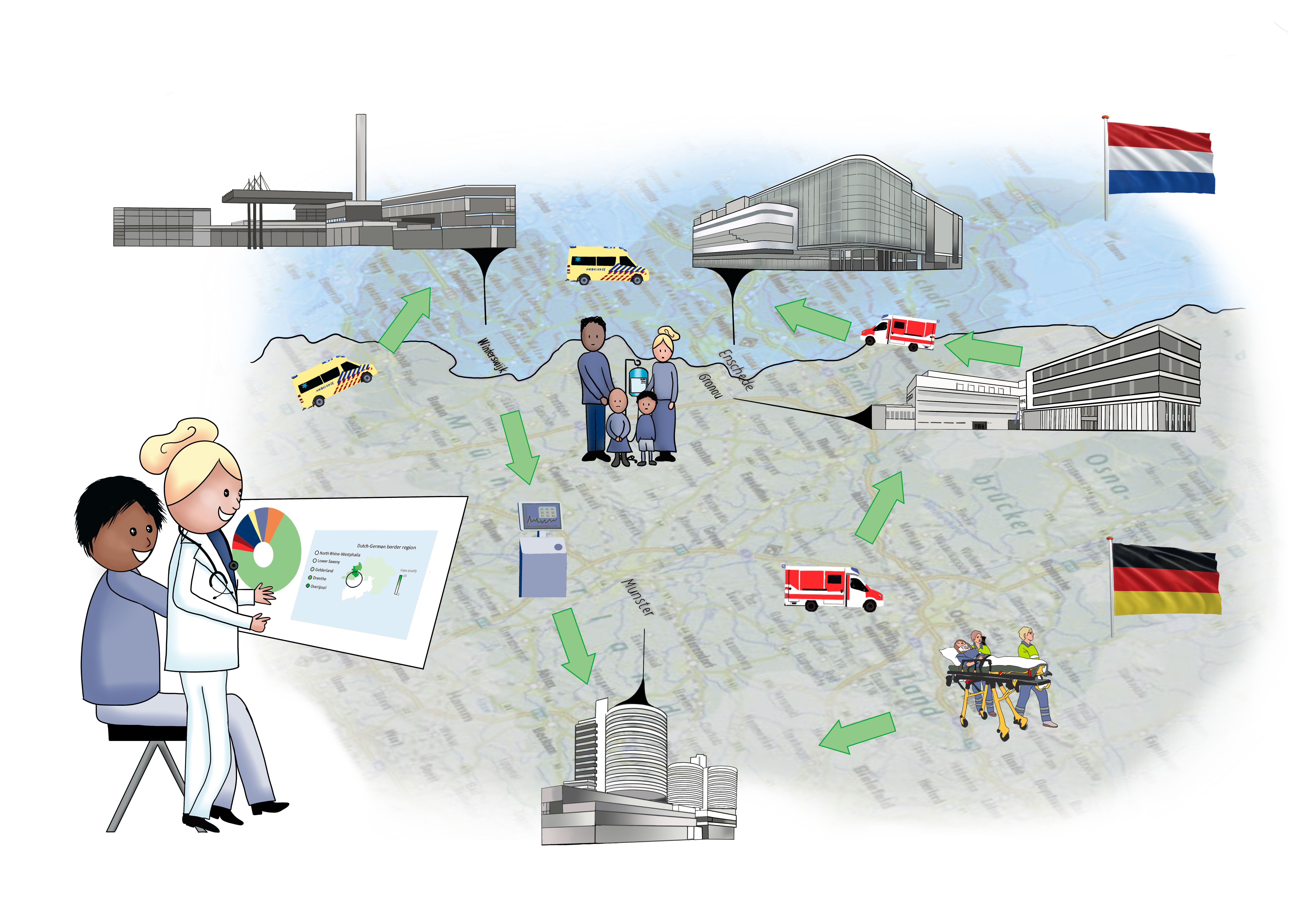
“Why should we adhere to national boundaries in this?” asks Fischer. “Suppose you have a very sick child with leukemia. You live in Enschede and drive two hours to Utrecht for every treatment. If we work across borders, the child can get the same treatment in Münster, which is only an hour away.”

An umbrella platform
Resource pooling is already taking place in the German-Dutch border region. Hospitals exchange helicopters and ambulances and distribute emergency and acute pediatric care. However, these projects are organized separately, and cooperation is based on bi-lateral agreements.
Fischer: “The resource pooling that takes place now depends on personal connections, on doctors or other professionals who know each other. It is not systematic, and there is no overview of what is available where. Moreover, the organizations involved experience enormous administrative burdens. You would think that the Netherlands and Germany are EU members, so organizing cross-border healthcare is easy. But sharing resources, patients, and staff is extremely complicated.”
A showcase to change policy
When Fischer began the research proposal, she and her team planned to develop an umbrella platform for medicine, equipment, personnel, and transportation. Soon, they realized that was unfeasible. “Take medications; all hospitals have stringent contracts about which medications they buy from which provider. But also consider insurance for patients abroad or specialized medical equipment doctors need to perform surgery.”
A comprehensive platform used in multiple regions is still the ultimate goal but for the long term. “Vincent Hofbauer, a colleague from the University of Münster, called it an eBay for healthcare”, Fischer goes on to say. At BRIDGE, the focus is on a platform for flexible staffing and flexible treatment locations for patients. “That should be the showcase, with which we can demonstrate to policymakers that this works. Because to allocate other resources more flexibly, policies have to change.”

Removing heavy burdens with technology
The project will start this spring. First, the researchers will analyze precisely what hospitals need and what the platform should look like. Then, NovioQ will build a low-code platform that is easy to use. “Anyone with minimal digital skills should be able to get along with it. Hospitals should be able to adapt it to their needs easily,” Fischer explains. If all goes well, the four hospitals involved will start using a pilot version of the platform early next year.
Whoever hears Fischer discuss her research and the BRIDGE project sees a passionate scientist. Her enthusiasm is contagious. Yes, there are numerous challenges, but most of all, the assistant professor sees many opportunities. “I truly believe that technology can lighten the heavy burdens the sector currently carries. It offers many opportunities to organize the healthcare sector better and more efficiently. I find that very hopeful.”