
By Michiel Verplancke. Fifteen international partners have joined forces to develop an exoskeleton for children with cerebral palsy. The complex skeleton will help them learn to take steps and learn how to walk. Until now, these kinds of exoskeletons only existed for adults. The MOTION project aims to change this.
More than 1 in 600 children are born with cerebral palsy. About half of them cannot walk without using aids. The muscles of these children are still functional in principle, but their brain’s control over them is faulty. There are also a lot of children who develop cerebral palsy later in life due to e.g. a tumor, a stroke, or some kind of trauma. It is these children that the researchers want to help with the project ‘Mechanised Orthosis for Children with Neurological Disorders,‘ or MOTION for short.
Easier training
“We focus on children between the ages of 8 and 12,” explains Prof. Luc Labey from the Department of Mechanical Engineering at KU Leuven (Belgium). “Given that the problems they have are primarily to do with the control of their muscles, we think that our exoskeleton can be of great help. The brain and nervous system are very pliable organs.”
“By practicing a lot and correcting their movements as you go along, you can basically improve control over your movements. But the training is physically and mentally difficult. Many children stop trying to take steps as they get older and wind up in a wheelchair. With an exoskeleton, they can practice in a more fun way.”
 Katrin van Herpe confirms this. She is a doctor who is specialized in physical medicine and rehabilitation. She works with children with cerebral palsy on a daily basis at the Pulderbos children’s rehabilitation center and knows perfectly well where the challenges and opportunities lie.
Katrin van Herpe confirms this. She is a doctor who is specialized in physical medicine and rehabilitation. She works with children with cerebral palsy on a daily basis at the Pulderbos children’s rehabilitation center and knows perfectly well where the challenges and opportunities lie.
“Therapists have to pay attention to an incredible number of things when supervising children who are impaired in their motor skills,” she knows from experience. “You have to hold the child upright, not drop it, put one leg forward, but also pay attention to the other leg. This is very stressful for the child and the therapist. In the hour that the therapist can treat the child, it ultimately ends up taking disappointingly few steps. That is very demotivating. This new technology will give the therapist the opportunity to concentrate on the step function and the step pattern, without having to keep an eye on all the other peripheries.”
Existing exoskeletons too heavy for children
Exoskeletons are a hot topic. They have been around for adults for a long time and have already yielded great results. So, why don’t children rehabilitate using exoskeletons? “The exoskeletons that are currently available are very heavy,” says Van Herpe. “Not only are children smaller and lighter than adults, but they also vary a lot more in height and weight amongst themselves. You can make small, medium, and large exoskeletons for adults, as it were. But for children, you need more customization. Both for the parts that we use to attach the exoskeleton to the body and for the operation of the motor.”
What’s more, the current exoskeletons are usually intended for people who can’t walk at all, which effectively makes it easier to control the suit. “The motors should barely respond to the behavior of disabled patients,” Labey explains. The robot takes over the step motion. All the patient does is move their center of gravity to indicate which leg needs to move. The target group that we have in mind is still able to take steps. In order to keep their muscles active, this new exoskeleton assists their gait pattern instead of taking it over. Because if the exoskeleton breaks with the gait pattern of these patients, there is a risk of muscle injuries or even falls.”
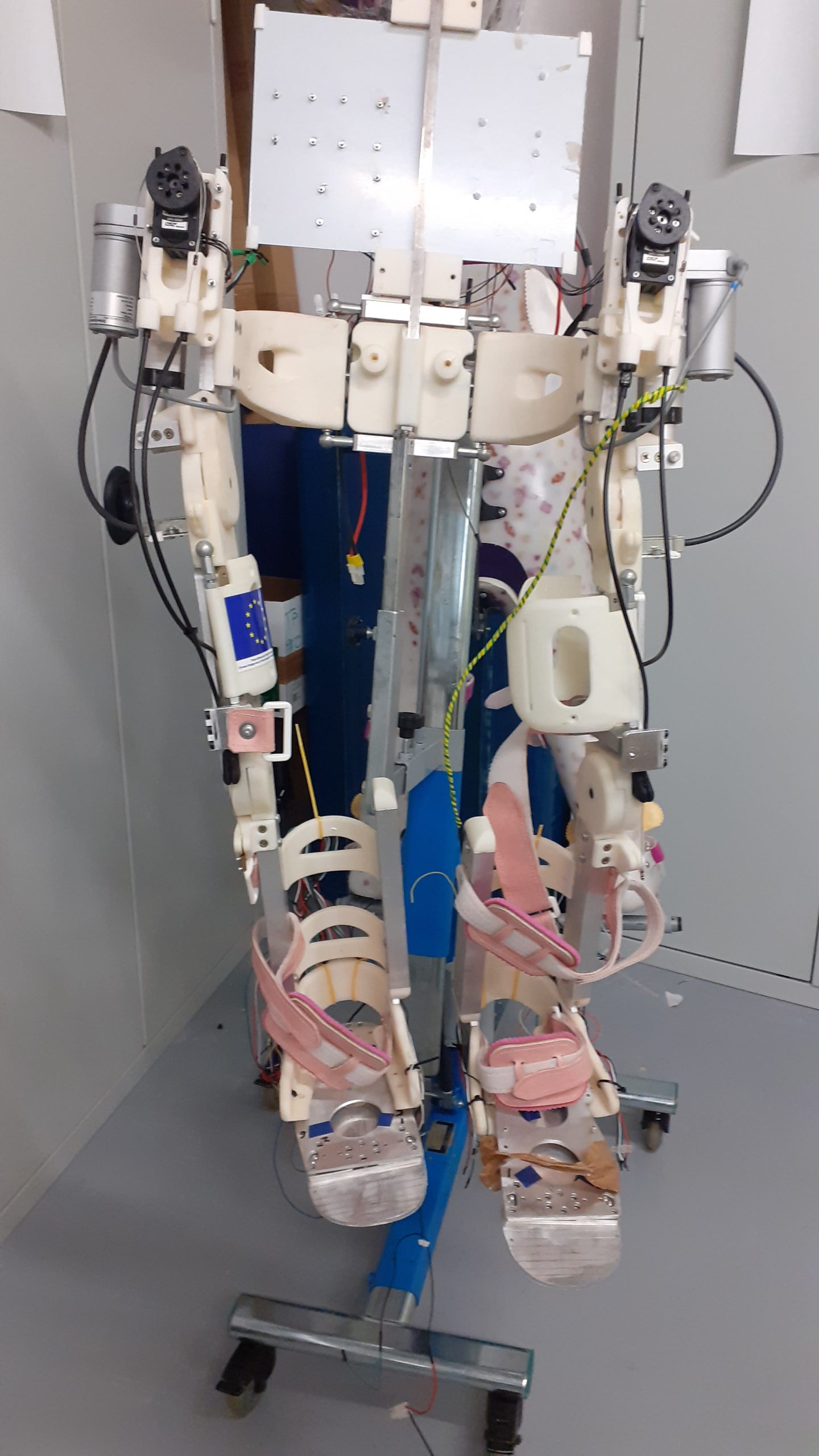
Three-piece exoskeleton
During the first phase, the researchers will divide the work up between themselves. Mobilab & Care of the Thomas More University of Applied Sciences (Belgium) is working on a powered ankle-foot orthosis. KU Leuven is focusing on a hip exoskeleton. The French engineering school HEI is building the frame and the complete exoskeleton. The University of Kent (United Kingdom) is tackling electronic hardware and control.
They do this not only to save time but also because some children have already been helped with a segment of the skeleton. “Our target group is very wide-ranging and all have problems with taking steps to a greater or lesser extent,” says Labey. There are, for example, children who mainly have a problem at their ankle joint, where the ankle orthosis may already be able to provide enough help.
Correcting the step pattern
Therefore, the different modules have the task of correcting the step pattern. To this end, the researchers are looking at various datasets that the UZ Leuven Pellenberg rehabilitation center has collected over the years. An ankle and a hip bend and stretch to a certain rhythm during the gait pattern. By comparing the typical gait patterns of children with cerebral palsy and those of their peers with a normal gait, they hope to determine the variances that can be seen at any moment while walking. The motor on the joint then adds the missing muscle strength to adjust the hip or ankle to the correct angle.
“To do this, we work with a number of ‘gait events,” Labey continues. “One example is when you make contact with the ground. That ‘event’ marks the transition from the swing phase to the support phase. You need to know exactly where the child is in the gait cycle at all times to be able to calculate the correct angle of the hip. But of course, the gait pattern in our patients is atypical. They are not making the right angles.”

“For example, someone with a pointy foot won’t hit the ground first with their heel, but with their toes. That means that a pressure sensor on the heel will not detect contact with the ground, but instead with a device on the lower leg that registers the movement, think in terms of a gyroscope.”
It’s a challenge to track those gait events reliably enough so that the algorithm can also detect a disruptive gait pattern. The events alternate in a matter of milliseconds. If you intervene too late, the patient will fall.
Taking steps is more difficult than it seems
“Taking steps looks easier than it is in reality,” says Van Herpe. “The brain has to direct an incredible amount of muscle to tighten and relax at the right time.”
At a later stage, the researchers will link the separate parts together into a single exoskeleton. The isolated motors will have to ‘talk’ to each other to determine exactly where the problem lies and how much power needs to be given. The University of Kent is figuring out what the role of artificial intelligence can be in the design of a control model.
According to Van Herpe, the three technologies will have a range of speeds and serve different purposes. “The exoskeleton will be used by therapists mainly during therapy. The ankle orthosis, on the other hand, is something that patients could also take home with them. So they can practice at home and keep on moving.”
Children who use the ankle orthosis already wear a lower leg splint. Except there is no movement in it. If you fix a leg at an angle of 90° to the ankle, the calf muscle can no longer do very much. If you keep some freedom of movement around the ankle and attach a small motor to it, the muscle will be able to move again.
“Imagine a lower leg splint as a kind of a ski boot,” Van Herpe explains. “You can walk in it, but it’s very awkward. You don’t have much freedom of movement. Imagine that the ski boot just moves with your foot and also adds energy at the right moment. This is what we are aiming for.”
‘Every child needs freedom of movement.’ Katrin van Herpe, doctor
Being able to take the full exoskeleton home with you is still a long way off. Then the researchers will need to take into account a variety of surfaces and obstacles and tinker around more with the safety aspects of the suit. Not to mention sorting out funding and the cost price. But Van Herpe does have high hopes. “Children with brain injuries have muscles that tend to shorten rather quickly, and their joints are more difficult to stretch. That’s why we ask them to stand in a standing device for one hour each day. There are wheels on it to move it around, but my hope is to be able to replace it with an exoskeleton someday. A child needs freedom of movement. Not only from an anatomical point of view but also to explore the world.”
Comfort has priority
The engineers who are developing the suit work very closely with the rehabilitation centers in order to understand exactly what the children and therapists need. And the most important conditions that they set are comfort, user-friendliness, and safety. “If a child wants to do something, it doesn’t have a lot of patience. Young children find it difficult to wait, especially if they are excited,” Van Herpe notes. If it takes half an hour to put on the suit, half the children are already done with it.”
What’s more, children have to feel good about themselves before they are able to really rehabilitate. “Children with cerebral palsy have been through a lot in their lives,” Van Herpe continues. “We attach great importance to building a bond of trust. That’s why it’s also important that the children feel good about that exoskeleton. How safe is it? How comfortable? An exoskeleton like that looks impressive. Their legs are not listening well to their brains, and now they have to deal with actions by a machine too. That can be stressful.”
The researchers have also come up with something for that. They are designing a smart textile that fits into the exoskeleton. By measuring ECG signals, heat generation, and sweat production, therapists can monitor whether the children are feeling any stress in the suit. On top of that, the textile uses EMG signals to measure muscle activity. Engineers can make improvements to the controls of the exoskeleton on the basis of these signals.
First trials early 2021
The first tests with the ankle orthosis on healthy people already turned out to be favorable. Detection of gait events seems reliable and robust enough to cope adequately with any deviations. And the first tests on patients? “They could start in the fall of 2021,” says Labey. “Although the corona crisis may have delayed a few things. We will first test all of the modules separately and then go back to the drawing board for the full exoskeleton.”
“I already have a few children in mind who would be helped by the exoskeleton,” Van Herpe looks to the future. “If the exoskeleton allows us to start rehabilitation faster and take more steps, we can make a fundamental difference to these children. Especially in children who suffered brain damage later in life. You recover fastest in the first days, weeks, and months after a brain injury.”
And the target group doesn’t have to be limited to children with cerebral palsy. The application will also be able to help children with spinal cord paralysis or a serious muscle disorder. “Exoskeletons are highly advanced technology,” Labey concludes. “If we can add value and force a breakthrough here, we will be taking a very big step forward.”
Related Posts





